How does MDMA work?
The brain has more than a passing similarity to a computer: It gathers information, processes it, stores it, and produces output. Just as different parts of your computer do different jobs, different parts of your brain do different jobs: Some areas of the brain decide what it is you’re looking at, some parts manage how you move your body in order to be able to walk, others turn your thoughts into spoken words and so forth.
As it works, signals fly back and forth, millions at a time, at up to the speed of sound. Besides the ‘task-specific’ regions of the brain, there is a vital system of controls that keep all these subsystems working and synchronized: The modulatory networks.
A modulatory network is a bunch of nerves in your brain that, instead of doing work themselves (like figuring out how to do a math problem) act as control centers, altering how the different parts of the brain work. Think of them as that pushy boss you once had that didn’t seem to really do anything himself, but was always running around telling everybody else what to do. While you may not have had much use for that boss, your brain really does need and benefit from these modulatory networks: When working normally, they keep mental traffic moving smoothly. The modulatory networks wake us up, put us to sleep, make us dream, and so forth. Although they don’t process information themselves (in the traditional sense), they are vital for our state of mind, including our emotions, alertness, etc. There are four major modulatory networks in your brain: Serotonin, dopamine, norepinephrine, and acetylcholine.
Serotonin
Perhaps of the most interesting of these modulatory networks is the serotonergic system. This network of nerves sends messages to the rest of your brain by releasing (or withholding) a chemical called serotonin. Serotonin is important for managing mood, appetite, sleep, and dreaming. If your serotonin levels become low, you may become irritable, anxious, depressed, and have trouble sleeping. The opposite is also true: Antidepressant drugs like Prozac, Paxil, Zoloft, etc. work by increasing serotonin levels, and by doing so often relieve anxiety, depression, etc. Serotonin can have both stimulant and sedative effects.
Beyond your mood, serotonin helps control the flow of thoughts and information in your brain, a little like a a cop directing traffic at a busy intersection. When the serotonin system is strong and active, thoughts flow in a fairly orderly, coherent manner. If serotonin levels greatly drop, thoughts become more scattered and unfocussed. Memory and concentration begin to suffer. Many a person under severe stress knows this feeling of ‘thoughts racing through your head, out of control’.
One particularly interesting role of serotonin is during sleep: When you are in REM sleep (the time when most dreams occur) the serotonin system turns itself off. Chaos reigns, thoughts run wild, vivid fantasies and nightmares emerge. The level of control is so low that the brain starts to generate its own dream sights and sounds and feelings without even needing outside input. While it might not seem relevant to know where dreams come from to a drug user, consider this: Drugs like LSD suppress the serotonin system. LSD can essentially activate your brain’s dreaming mode while you are still awake!
Many popular ‘psychedelic’ drugs work by affecting your brain’s serotonin system.
Outside the brain, serotonin promotes the contraction of smooth muscle. Smooth muscle is the kind of muscle that lines our digestive tract and blood vessels. As a result, drugs that act on serotonin can often cause an upset stomach and increases in blood pressure. (One of the more potent serotonergic drugs, DMT, commonly causes vomiting and diarrhea in users when used in an oral form called Ayahuasca.) Most of your body’s supply of serotonin is actually in your blood cells, which, through its vasoconstrictive properties, use it to affect blood flow.
MDMA (“Ecstasy”) works primarily by releasing very large amounts of serotonin.
Dopamine
The dopaminergic system is a little less mysterious than the serotonin system, but still of great interest to drug users and scientists alike. Dopamine is most famous for its stimulant and pleasurable effects, and appears to be important in learning. The popular drug Ritalin (prescribed for attention-deficit/hyperactivity disorder) works by elevating dopamine levels, making the user more focused and interested in what they are doing. Drugs that significantly elevate dopamine levels tend to make people euphoric, confident, aggressive, and hyperactive.
Highly elevated dopamine levels are associated with some mental illnesses, such as schizophrenia. Prolonged abuse of amphetamines can produce temporary psychosis (losing touch with reality). By the same token, very low dopamine levels also cause problems–the symptoms of Parkinson’s disease are caused by the loss of dopamine neurons.
In the opposite direction, drugs that can suppress dopamine (Xanax, Valium, Rohypnol, GHB, alcohol, etc.) are sedating, at high doses causing loss of consciousness and amnesia. As a result of their effects, illegal dopamine suppressing drugs have gained a reputation as “date rape” drugs. While they can be used for that purpose, there is no evidence that such crimes are common (or begin to approach even a small fraction of the number of cases of alcohol-facilitated rapes.)
Because they are pleasurable, drugs that strongly elevate dopamine levels tend to be very powerfully ‘re-enforcing’ (meaning the user is often highly motivated to continue use). Of prohibited drugs, the most famous examples of dopamine elevators are amphetamine, methamphetamine, and cocaine. Among legal drugs, the nicotine in cigarettes causes the release of dopamine (among other things.)
Unlike serotonin, the dopamine system doesn’t undergo major cyclic shifts in activity levels during the course of the sleep/wake cycle…it continues to operate at a more-or-less constant level throughout the day and night.
MDMA releases a moderate amount of dopamine.
Norepinephrine
Also called “noradrenaline”, norepinephrine is similar to dopamine in that it also produces alertness, focus and motivation. America’s favorite daily drug, caffeine, releases norepinephrine, helping you get going in the morning and stay mentally sharp. Norepinephrine doesn’t appear to be nearly as strongly re-enforcing as dopamine.
MDMA releases large amounts of norepinephrine.
(Of prescription drugs affecting norepinephrine, one of the more interesting ones is Modafinil, a stimulant that in Canadian military experiments was able to keep people awake and mentally sharp for days without sleep.)
Acetylcholine
Within the brain, the cholinergic system is suppressive (parasympathetic.). That means when acetylcholine levels rise, the brain generally becomes less active; nerves are less able to ‘fire’. This system becomes active during sleep, and may be responsible for disconnecting the brain from the body (so you don’t actually try to run when you dream that you’re running.)
MDMA does not appear to significantly affect acetylcholine.
Outside the brain, acetylcholine has a critical role: It’s used by nerves to tell striated muscles to contract. Striated muscles are what people normally think of as muscles…your biceps, etc. Because of this effect, drugs that block acetylcholine receptors (such as curare) can paralyze and kill (by stopping breathing and the heart.) Chemicals that prevent the breakdown of acetylcholine (nerve gas and some insecticides) are also dangerous; as acetylcholine levels rise out of control, muscles can go into spasms, causing heart attacks and difficulty breathing.
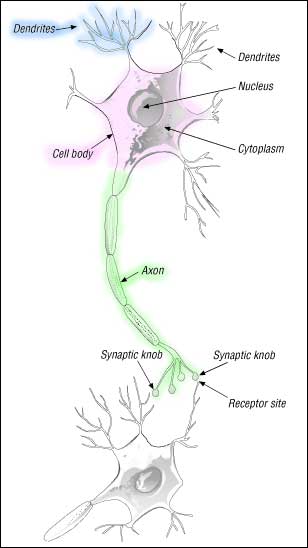
The Axon: Relatively thick and often very long ‘cables’, axons are the transmitter towers of the neuron–they send out signals to other neurons.
The Dendrite: Thin, moderately long projections, dendrites act like antennas–they pick up signals sent by other neuron’s axons.
Cell Body: The big central part of a neuron is called the cell body. It contains the cell’s nucleus, DNA, and all the mechanisms cells need to live and work. Like dendrites, the cell body can receive signals from axons that are in contact with it.
Although there are neurons everywhere in the brain, the modulatory networks (such as the serotonin system) have their own home areas: They live in clusters in the brain stem called the raphe nuclei. From their home in the brain stem, the serotonin neurons send long, highly branched axons out to the rest of the brain:
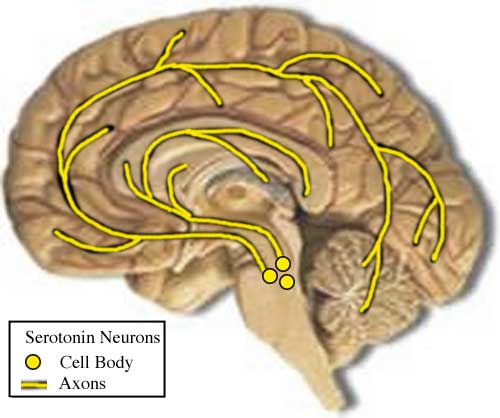
In this picture, the size of the serotonin neurons has been greatly exaggerated; there are several hundred thousand serotonin neurons in the human brain, operating vast networks of fine axons. The serotonin axons ‘curl around’ the brain instead of spreading out straight because of how the brain develops. (The modulatory networks are evolutionarily ancient, seen in the brains of all vertebrates…the parts of the brain that can tell a dirty joke or order a pizza were added on relatively recently.)
Call me!
When one neuron wants to talk to another, it tells its axon to send out a signal. This signal is sent by releasing a chemical called a neurotransmitter. Types of neurons are named for the type of neurotransmitter they use. For instance, dopamine neurons use the neurotransmitter dopamine to signal other neurons, serotonin neurons use serotonin, and so forth.
The place where an axon meets up with another neuron is called a synapse. In a synapse, a small open space separates the two neurons. Technically this gap between neurons is called the synaptic cleft, but people usually just call it ‘the synapse.’
Let’s take a closer look at the structure of a synapse:
That looks like a mess, but we’ll take it one step at a time. The new players:
• Vesicles: These are temporary storage tanks for neurotransmitters. You can see one vesicle being dumped into the synapse to signal the second neuron.
• Receptor: These are the actual ‘sensors’ that detect a neurotransmitter. Each type of receptor has a different shape that fits a different neurotransmitter, like a key in a lock. One of the receptors shown here has been ‘turned on’ (activated) by the right neurotransmitter fitting into it. What the neuron will do in response to one of its receptors being activated varies…often it will cause the neuron to fire (release its own neurotransmitters to signal even more neurons.)
• SERT: The Serotonin Transporter. Rather than just let the neurotransmitter escape and be wasted, the axon uses these little pumps to suck it back up and reuse it.
So, the whole cycle is:
1. An axon releases neurotransmitters into the synapse.
2. The neurotransmitters fit into receptors, activating them (delivering the signal.)
3. The transporter (SERT in the case of serotonin) pumps the released neurotransmitter back into the axon for reuse.
This process isn’t perfect…some of the neurotransmitter will escape, but not much under normal circumstances. To replace what does get away, the body is continually making more.
How much/how often neurotransmitters are released determines how strongly the neuron on the receiving end will be affected. If only a little serotonin is released, you may feel irritable, anxious, or even depressed. On the other hand, if a lot of serotonin is released you will probably feel calm, relaxed, and happy.
MDMA works primarily by causing the serotonin axons to release a lot more serotonin than they normally would. As the amount of serotonin in the synapse increases, the rate of serotonin receptor activation increases…and you start to feel different, and probably very good.
The downside is that, by forcing a lot of your serotonin to be released (and interfering with the SERT’s ability to get it back) a great deal of serotonin escapes the synapse and is broken down in your body. Given time (it may take days, even a week or so) your body will replace the lost serotonin (see the 5-HTP section in Preloading). In the meanwhile, however, your brain may not be able to release as much serotonin as it wants to, causing irritability, anxiety, and other symptoms. Taking 5-HTP to quickly replace serotonin is a very useful tool to prevent such side effects following the use of MDMA.
MDMA affects dopamine and norepinephrine neurons in much the same way.
MDMA at work
When MDMA reaches the brain, it sticks to the serotonin transporter and keeps it from working properly, allowing serotonin to leak out of the axon and keeping it from being recovered. (Antidepressants like Prozac keep MDMA from working because they block its access to the SERT.) As serotonin (and dopamine and norepinephrine) levels rise, you start to feel high.
Neuroadaptation (or, Where E-tards (usually) Come From)
Your brain doesn’t just take getting kicked around by drugs sitting down. Your brain is constantly trying to maintain ‘normal’ levels of activity from these different systems; if one system throws a big party (with the help of MDMA), your brain will try to turn the volume down on that system by removing some of the receptors that (for instance) all that excess serotonin is activating.
This system of neuroadaptation is the basis of physical dependence and drug tolerance; when your brain is frequently exposed to a drug it adapts to compensate for the presence of the drug. As a result, if the drug is taken away, it leaves your brain ‘overcompensating’ and off balance in a new way. If you frequently use a drug that suppresses anxiety, then go off it suddenly, you are likely to experience ‘rebound’ anxiety. If you take a lot of pain killers, then go off them, you are likely to experience ‘rebound’ pain, even if nothing is wrong with you.
Neuroadaptation isn’t ‘strange’ or abnormal; it’s something that is always going on, with or without drugs. It’s the reason we develop a tolerance to caffeine…and why that tolerance goes away if we give up caffeine for an extended period.
Neuroadaptation isn’t limited to changing the existing receptors. Neurons can also adapt by producing more or less of enzymes that break down neurotransmitters or drugs, or by producing more or fewer new receptors over time. (Proteins like receptors are constantly wearing out and being replaced; thus, if the neuron produces fewer new receptors, the number of receptors will go down over time.)
In the case of drugs like MDMA, use temporarily alters your brain’s sensitivity to serotonin. If you use heavily, these changes start to add up as your brain continues to work to counteract the drug effect. As a result, periods of heavy MDMA use can leave your serotonin system hardly knowing if it’s coming or going; it doesn’t quite work as it should when you’re high, and it doesn’t quite work as it should when you’re sober. The result is often anxiety, depression, memory problems, lack of motivation, and feelings of emptiness. This is the real reason you shouldn’t use MDMA frequently; the aftermath of the more impressive binges can be quite disruptive to your life and sometimes lasts for months.
This graph shows the effect of a very large dose of MDMA (up to 20 mg/kg twice a day for four days) on the number of available serotonin receptors in the brains of a group of rats: [5]
After the last dose of MDMA was given to the rats, their neurons had deactivated most of their serotonin receptors; over the next 3-4 weeks, the process slowly reversed itself, and the receptor density returned to normal. In the meanwhile, these rats might have felt a little strange.
Now, let’s imagine what this effect might look like in a human MDMA user’s brain as they go from infrequent to frequent use:
Given enough time, the brain’s sensitivities return to normal (human research suggests this takes about 3-4 weeks after a single moderate dose.) However, if additional doses are taken before this recovery occurs, the changes can be made greater, increasing the symptoms it might cause and taking even longer to recover from. People seem to vary in their sensitivity to frequent use; some rare people claim that once-a-week use for prolonged periods hasn’t had a major negative impact on them, while others have felt a little irritable and ‘off’ even with just once-a-month use. Pay attention to your mental state; if you start to feel a little irritable or otherwise emotionally unstable the week after use, cut back on your usage.
The only cure for such neuroadaptation is time, although treatments that support the serotonin system may help with symptoms (SSRIs, 5-HTP.)

The Neurotoxic Question
Of course, recovery depends on not having done any real damage in the first place. MDMA is well known for it’s potential neurotoxicity (ability to damage neurons.) If neurotoxicity occurs, then the slow reversal of neuroadaptation isn’t enough to truly restore your brain to its pre-use state. Repeated or large doses of MDMA may cause permanent harm, not just transient neuroadaptation. MDMA’s neurotoxic potential (and it’s implications for human users) is a complex subject, but is covered in detail on this site’s Neurotoxicity page.
The short version is that the more you take, the greater the risk. I advise against taking more than a single oral dose in an evening, and never mix with amphetamines. MDMA neurotoxicity is not an all-or-nothing issue; just because you’re taking some MDMA does not mean you have nothing more to lose by upping the dose; if anything, the second dose in an evening may be more dangerous to you in terms of neurotoxic potential than the first dose.
For further reading on transporter mediated exchange and MDMA, see:
[1] Rudnick G, Wall SC “The molecular mechanism of “ecstasy”; Serotonin transporters are targets for MDMA-induced serotonin release” Procedings of the National Acad Sci (USA), 1992; 89:1817-1821. Abstract
[2] Gu XF, Azmitia EC “Integrative transporter-mediated release from cytoplasmic and vesicular stores in cultured neurons” Eur J Pharmacol, 1993; 235(1):51-7. Abstract.
[3] Wichems CH, Hollingsworth CK, Bennett BA, “Release of serotonin induced by 3,4-methylenedioxymethamphetamine (MDMA) and other substituted amphetamines in cultured fetal raphe neurons: further evidence for calcium-independent mechanisms of release” Brain Res. 1995; 695(1):10-8. Abstract.
[4] Crespi D, Mennini T, Gobbi M, “Carrier-dependent and Ca(2+)-dependent 5-HT and dopamine release induced by (+)-amphetamine, 3,4-methylendioxymethamphetamine, p-chloroamphetamine and (+)-fenfluramine” Brain J. Pharmacology, 1997; 121(8):1735-1743. Abstract.
[5] Scheffel U, Lever JR, Stathis M, Ricaurte GA “Repeated administration of MDMA causes transient down-regulation of serotonin 5-HT2 receptors” Neuropharmacology, 1992; 31(9):881-93. Abstract.
[6] Ravma AW. Sylte I, Dahl SG “Molecular model of the neural dopamine transporter” J Comput Aided Mol Des., 2003 May-Jun;17(5-6):367-82. Abstract.